TOOTH RESORPTION
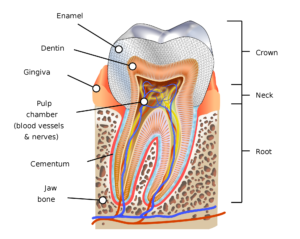
Tooth resorption is the progressive loss of dentin and cementum by osteoclasts. Dentin is the tooth layer under the enamel and covers the pulp chamber. Cementum is the surface layer of the tooth root covering the dentin. Osteoclasts are bone cells that break down bone tissue.
There are two kinds of tooth resorption: Internal and External
Internal- very rare
- Lesion always centers in x-rays
- Requires vital pulp
- Cannot trace the root canal through the lesion
- For resorption to continue there needs to be a vital pulp-once the pulp is removed the resorption stops
- Has a pink spot in the tooth caused from inflammation and hemorrhaging-depending on the stage of resorption is how much the pink shows

Treatment
- RCT -will stop resorption
- Internal whitening is recommended after RCT
External – more common
- Will move with angle of x-ray —if lesion moves to the mesial on the x-ray the lesion is facially
- May or may not have a vital pulp
- Can continue after RCT or pulp is removed
- Can still trace the outline of the root canal
TYPES OF EXTERNAL RESORPTION
Inflammatory
- Almost always from trauma
- Can show up quickly after trauma or years later
- Needs to be followed for life
- Recommended a PA type of radiograph one time a year
- May or may not have symptoms
- Can continue after pulpal necrosis
- Loss of bone usually close to lesions
- Outline of root canal is still there
Treatment
- Root Canal Therapy
- Calcium Hydroxide — strong antimicrobial as an intra-canal medicant. This increases pH of dentin to inhibit activity of osteoclasts. Osteoclasts destroys and attacks tooth structure with an acidic pH. Calcium hydroxide takes four weeks for pH to change and bring resorption to pH 11.
- For best results 7-10 days is the timeline to have avulsed tooth Root Canal Therapy.
Surface or pressure related
- Ortho – retention. Maxillary laterals most common area
- Coronal – example: a wisdom tooth hitting on the tooth in front of it
- Peri-radicular – example: impacted canine
- Apical – on the root of the tooth
Replacement or Ankylosis
- Tooth structure replaced with bone that fuses with dentin
- Frequently after avulsion with extended extra- oral dry time
- Tooth out of occlusion usually facially angled
- Tooth usually has NO movement, where all teeth tend to have slight movement. It’s like tooth is in cement
- When tapped it has a high pitch metallic sound, the same as an implant sound
Treatment
- Extraction immediately, sometimes may have to grind out the tooth
- If the tooth is out of the mouth for awhile fluoride may help to prevent ankylosis before putting the tooth back in the mouth
- Flexible splinting may help also
Invasive Cervical (ICR)
- Starts in cervical area but can extend apically to involve the entire root surface
- May have a pink spot
- Can trace the root canal through the lesion
- Usually isolated tooth and not multiple teeth
Causes
- Trauma (not common)
- Developmental defect
- Viral etiology
- Idiopathic
Four classes:
Class 1 – small invasive resorptive lesion near the cervical area with shallow penetration into the dentin
Class 2 – a well-defined invasive resorptive lesion that has penetrated close to the coronal pulp chamber but little or no extension into the radicular dentin
Class 3 – a deeper invasion of dentin by resorbing tissue, involving the coronal third of the root
Class 4 – a large invasive resorptive process that has extended beyond the coronal third of the root canal.
Keep in mind, tooth resorption, doesn’t have any symptoms. No pain is related to it, so taking annual radiographs are very important to find this issue. Honestly, I haven’t come across resorption too often in the years I’ve practiced dental hygiene. But I just took a continuing education course on it and found it very interesting and important to share, so you’ll be aware of this issue if this happens to you. Also, I want to stress the importance of having this taken care of sooner than later to preserve the tooth.



{kind=link}
{kind=link}
{kind=link}